
ADHD Awareness Month
by Jack Hellberg, DEN co-chair
Hello everyone. Increasingly, I have seen discourse online and the media turn its focus on rising diagnostic rates for neurodivergence. This is a significant and important topic, as diagnostic services are under significant strain and medication supplies are often unable to keep up with demand. Around the diagnostic process, our understanding of neurodivergence is certainly incomplete and diagnostic criteria will undoubtably continue to change over time. However, there is a common attitude that I encounter that “everyone is just neurodivergent now” or “anyone can get an ADHD/Autism diagnosis”. Anecdotally, people often ask me something along the lines of “what do you think about all these people claiming they are neurodivergent on TikTok” when they learn that I work for an adult autism assessment service. In response to this, I would like to outline my thoughts on why ADHD diagnostic rates in adults specifically are on the rise:
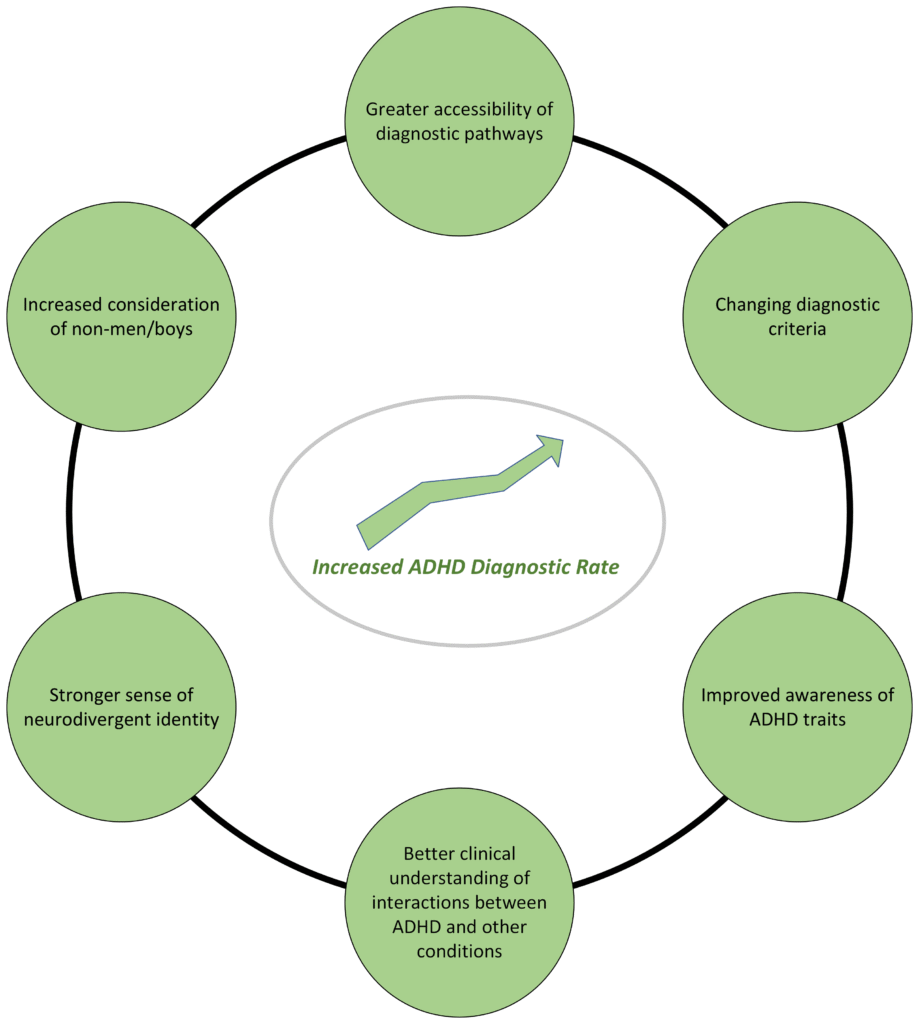
1. Changing diagnostic criteria
The DSM-5, published in 2013, outlines the diagnostic criteria clinicians use to evaluate someone for ADHD. These criteria require a variety of traits which broadly fall into one of three varieties (predominantly inattentive, predominantly hyperactive-impulsive, and combined) and some evidence of traits prior to 12 years old. However, this has not always been the case. From 1994-2013, ADHD-type categories were not only more rigidly defined, but there must also have been proof of traits prior to 7 years old. Due to these changes, we are finding many people were not eligible for ADHD diagnosis until the past decade.
2. Greater consideration for women having ADHD
There is a significant gap in diagnostic rates between women and men (3.9:1 according to one study). However, this gap used to be much larger and is in the process of shrinking. We can therefore see increasing ADHD diagnoses as a bit of “catch-up” as the artificially created gender gap in ADHD diagnosis begins to level out. This gap can be understood as a product of two primary factors. Firstly, historically ADHD was understood as a condition which was exclusive to pre-pubescent boys. However, even when girls became eligible for ADHD diagnosis, they often did not demonstrate traits in the same way. Non-boys/men are more likely to mask or suppress signs of hyperactivity or impulsivity, therefore not showing the “disruptive” behaviour typically looked for by educators and clinicians. While there is greater awareness of these gender differences, on average men might still have an easier time getting diagnosed than women. In any case, there is likely a large population of AFAB (assigned female at birth) people with undiagnosed ADHD who are now seeking an ADHD assessment now that they are more likely to be considered.
3. Wider knowledge of ADHD traits and a sense of neurodivergent community
Lastly, I would like to acknowledge the role of the internet and social media in the increased discussion of ADHD. Firstly, yes, I have no doubt that discussion of ADHD online has led to more people seeking an ADHD diagnosis. However, in my personal experience this has not resulted in waitlists clogged with people not fitting diagnostic criteria. Rather, I mostly encounter people who found social media content validated their long-standing observations about themselves to the point that they felt comfortable to pursue a diagnosis. Social media content about the experience of ADHD helps normalise ADHD traits and gives people the tools to advocate for their health. Additionally, content on social media has led to the rise of the neurodivergent community. People who are or suspect they are neurodivergent understandably want to engage with people who have similar experiences to them, especially when you consider the exclusion many of these people face in other settings. In this way, social media content surrounding neurodivergent experiences likely does increase demand for assessment services via increased awareness and confidence to pursue a diagnosis for those with lifelong neurodivergent traits.
I have only outlined a few of the factors contributing to higher rates of ADHD diagnosis. Neurodivergence generally is an area of rapidly evolving understandings and we will continue to see things change in the coming years. Due to recent changes, diagnostic criteria for ADHD is more equitable than ever before and more people have a general awareness of ADHD than ever before. Groups who have historically been excluded from accessing the healthcare services they need are now increasingly being considered by professionals. Overall, ADHD assessment services are effectively working through decades of backlog as people dismissed in their childhood are now being given the second look they deserve.
Disability Pride Month
by Emma Chalmers, DEN co-chair
For Disability Pride Month, the DEN co-chairs will post about their personal experience with disability. Come back next week for the next installment!
My contribution to the DPM blog series is going to talk about how being disabled changed my life, somewhat for the bad but mostly for the good.
I didn’t know I was disabled until 2021. Without giving too much about my age away, that did mean spending 30-odd years believing that I was non-disabled, that my fatigue was just shift related and that everyone dealt with overwhelm and pain all the time. It’s amazing how much we don’t listen to our own bodies when we should.
‘Becoming’ disabled was a real shock to the system. Not because I needed to change any habits of mine, but because I worked in a job that needed me to be mobile and active. And I just couldn’t. The day I told my boss that I might need to start using a wheelchair in work was one of my toughest days. I’m pretty sure I scared the poop out of him too as I was immediately referred to Occ Health. Clearly my masking had been working a little too well!
So, to why being disabled is bad AND good.
I’m sure you can imagine why it’s bad. I’m physically disabled with Ehlers-Danlos Syndrome, Functional Neurological Disorder, kyphoscoliosis and polycystic ovaries and I also have depression and likely ADHD (gotta love those waiting lists right?!). I had to grieve my life before. Grief for disabled people is huge. We say goodbye to a lot of what could have been, and grief needs to be done before we can accept and embrace what will be. Life is a series of balances; I have to balance my energy use, balance my work, balance my out of work activities. Just constant plate spinning. It’s exhausting. It’s overwhelming and it’s so much more than many people realise.
But it’s also given me so much. I got to learn who will be there for me. I’m sure you’re shocked to read that one of those who couldn’t be there for me was my husband (now ex). I discovered more of a found family than I had before. I learned to really listen to my body and what it needs, instead of just pushing through and making myself ill.
I got to move into a job that I absolutely adore. I did not expect that a job could be found for me that would both suit my physical needs but also that wouldn’t feel like being just put somewhere out of the way.
I would not have been as much an advocate for people as I am now without becoming disabled. It gave me the opportunity to become co-chair of the Disabled Employee Network, and I really love this work. I’m still helping others, like I did in my old life, but this time I can do it within my own capabilities, and I can help my disabled colleagues, you guys.
I have been able to learn so much more since becoming disabled. About myself, about disabilities, rights, service areas, things I enjoy doing and how to use my voice for the better.
So yes, I guess I do have pride in myself this disability pride month. Look at all I’ve done so far, and look at what I can do in the future. I’ll keep on going, because I’m looking so forward to seeing what else I can do and learn.
Disability Pride Month
by Jack Hellberg
July 2025
For Disability Pride Month, the DEN co-chairs will post about their personal experience with disability. Come back next week for the next installment!
Hello everyone. My name’s Jack and I am a co-chair of the DEN. I have written a few bits for the DEN, mostly around neurodivergence and the history of disability rights & advocacy. However, I realise now that I have never properly introduced myself and my relation to disability. For my first blog post in a while, I would just like to chat a bit about my own journey with disability and particularly the neurodivergent community means a lot to me.
I have ADHD, although I often suspect autism could be part of my neurodivergence as well. The possibility of ADHD was highlighted to me when I first lived with other people in my second year of uni. My flatmates noticed that I had to spend significantly more time working on assignments than them, getting up to pace or becoming distracted every 2-5 minutes. This had always been the way I worked, and I had always just blamed my own motivation for this. Through primary and secondary school, I remember frequently forgetting to turn in assignments which often got me in trouble. My teachers would always ask for an explanation for this difficulty, or flag that I just might not be trying hard enough. This was obviously upsetting, particularly as I felt that I was trying incredibly hard. It was validating to eventually be told that I likely had ADHD from the education psychologist I first saw. Knowing that made the things that are hard feel less like a personal failing. Today, I can still have a difficult time keeping everything organised (this very article has certainly been procrastinated a little bit!), but I am better able to practically and emotionally cope with this than before I was aware of my neurodivergence.
The neurodivergent community is a great place to be. It’s a safer place to be myself, and I can worry less about things like getting carried away talking about an interest or accidently interrupting someone. I don’t need to be monitoring whether I am making too much or not enough eye contact, and I can trust that the feedback I get from others is genuine. In my experience, the neurodivergent community is a place where people are given free rein to discuss what is important to them in the way that is most comfortable. There’s no pressure to perform a social role or stick to small-talk, which is exactly the environment which many neurodivergent people need. It’s our own unique culture, and for disability pride I would simply like to say thank you to the rest of the community for being a part of it.
Pride²
by Emma Chalmers, DEN co-chair
June 2025
Pride squared? Emma, are you confused?
Nope. In fact, I’m taking this opportunity to talk about two different but equally important Pride months. June has long been held as Pride month for the LGBTQIA+ community. The first Pride was no celebration, it was in fact a riot in America, in 1969, led by trans people, drag queens, and butch lesbians. How sad it is that 50 years on and we’re still fighting for trans rights, possibly even watching the positive momentum being dragged backwards by poor political stances and policy making. I’m not saying that we should begin another riot, but this is the time to use our voices to support our marginalised peers.
People don’t exist in a vacuum. We’re not ‘only’ gay, or ‘only’ disabled. I’d hazard a guess that a fairly decent proportion of LGBTQIA+ folks are also disabled, and so the intersectionality of discrimination is vital to analyse and discuss.
Have some stats from Stonewall UK-
- There is a higher rate of hate crime towards disabled members of the community
- 19% of disabled LGBTQIA+ members have had difficulty accessing healthcare
- 20% of LGBTQIA+ disabled people have faced discrimination in healthcare
- Many disabled people also struggle with their mental health at a much higher rate
- 8% of disabled LGBTQIA+ people had attempted suicide in 2018.
- 59% said life was not worth living at some point in comparison 31% of LGBTQIA+ who are not disabled
Life is not easy as a disabled person. Add to that being a person who is not heterosexual or cisgender, and you add to the stress and distress. Hate crimes against marginalised groups are not rare occurrences. They are under-reported and under-convicted but they still go on.
We in NHS Lothian have staff support networks for both disabled employees and our LGBTQIA+ colleagues. Sometimes, we get asks for support from people who are experiencing issues based on the fact that they are a disabled queer person. Which one do we focus on first? Neither; we need to address both as neither one is more important than the other, discrimination just can’t stand.
But so far, I’ve only mentioned the Pride held in June. Let’s look at July – Disability Pride Month. A newer ‘celebration’ but as I’ve said before, but no less important. Disability rights also began with riots, protests, arrests and generally ‘making a nuisance’ of ourselves. Look up the history of the UK’s Disability Discrimination Act 1995 (absorbed into the Equality Act 2010) and the US’s Americans With Disabilities Act (ADA). Neither started because some kindhearted people remembered our right to exist. They started much like Stonewall did – by screaming our rights from the metaphorical (and sometimes literal) rooftops!
What does Pride have to do with this? Well I, personally, don’t necessarily use the word pride as a descriptor when I talk of my disabilities. I’m certainly not ashamed but it isn’t the word that comes to mind. So what do I do during DPM? Well, I find my pride aimed at my advocation forerunners. They broke the ground of change for disabled people, allowing me to keep pushing the fight forward. And so, during DPM, I use that pride as a tool, and I metaphorically try to scream from those rooftops to keep our voices loud. And I suppose proud!
For those in the LGBTQIA+ community, both in NHS Lothian and outwith, as you come to the end of your Pride month, and to the beginning of mine, know this- DEN stands, sits, rolls and shouts with you. We got your backs. Keep with the fight!
World Cancer Day and International Childhood Cancer Day
by Emma Chalmers, DEN co-chair
February 2025
February is a month of awareness when it comes to cancer as we have both World Cancer Day on the 4th and International Childhood Cancer Day on the 15th.
Cancer is one of the biggest killers internationally, with estimations that 1 in every 2 people will be diagnosed in their lifetime. What is more promising though is that 50% of those people will survive to 10 years and beyond.
Cancer treatments have been around since when Marie Curie discovered Radium in 1898, and people began to be treated for skin cancers with this radiation. Since then, the treatment options for all cancers have grown exponentially with some of the more recent treatments being made from a patients own genetically modified immune cells. Clinical trials are consistently growing year on year to help find more and more effective treatments.
Cancer is not the life sentence that it was 50 years ago, and many people now live with it as a chronic illness.
There is no way to predict if someone will develop cancer in their lifetime, but we do know that 4 in 10 cancers are preventable with lifestyle modifications. The biggest is to not smoke or vape. Others include avoid drinking alcohol above recommended amounts, eating fresher foods and avoiding ultra-processed foods, reducing stress in our lives and keeping to a healthy weight (obesity is the 3rd biggest cause of cancer according to the WHO). Ways to reduce your risk also include having good cardiovascular health, so exercising regularly, and ensuring that your emotional wellbeing is being taken care of.
There are hundreds of supportive groups and charities for both patients and their loved ones, as well as for those of us who care for cancer patients in hospital, but I would recommend two personally, especially as there are physical locations to attend- Maggie’s (WGH, behind ward 1) and Macmillan (on the Main Corridor in WGH).
Cancer is still a big and scary diagnosis, but no one is alone.
ADHD Awareness Month
by Jack Hellberg, DEN co-chair
October 2024
October is about ADHD awareness, but many people with ADHD feel that it is not the whole story of their neurodivergence. Even for those who take medication, which can make some things easier to manage, there are other traits that leave lingering questions. Maybe you are particularly prone to becoming overstimulated, or paradoxically fall into periods where you are consumed by a single topic and yet cannot muster the focus to pursue it. Maybe you feel like you just have to get up and be active but, at the same time, cannot find the resources (or the spoons) to do so. For many people, ADHD answers some but not all of their questions about why they are the way they are. As our understanding of neurodivergence has rapidly changed, so too has the picture of the complex relationship between autism and ADHD.
Diagnostic recognition for ADHD and autism is a much more contemporary change than some might realise. It was not until the early 21st century where ADHD in adulthood gained widespread professional recognition. ADHD and autism were seen as mutually exclusive by practitioners until 2013. This left people with traits falling into both categories at a crossroads; which should they (or their practitioner) “pick” as a diagnostic label? For many, an ADHD diagnosis was the answer in order to access beneficial medication, but this naturally could leave them feeling that they still did not have an answer for many of their other differences.
Our understanding of the relationship between autism and ADHD today is in a transitional stage. 53-78% of diagnosed autistic people have some ADHD traits (Young et al., 2020), and 21% of people diagnosed with ADHD have some autistic traits (Hollingdale et al., 2020). While “traits” don’t necessarily cross the diagnostic thresholds to justify a second diagnosis, it is clear that co-occurring ADHD and autism is much more common than previously thought. However, many diagnostic pathways still stick strictly to one neurodivergence. In light of our growing understandings, single “neurodivergent” diagnostic pathways might be the answer. Additionally, the traits typically associated with ADHD and autism continue to overlap more and more. For example, social difficulties can now be seen as features of ADHD, and autistic people can have difficulty with focus, particularly at times of burnout.
Overall, the picture of ADHD and neurodivergence in general is rapidly changing. There are still common outdated and harmful beliefs about what ADHD looks like, and yet there is a lot of new evidence that might make us question our current understandings. What we currently classify as ADHD can present differently in different people with the same diversity that we see between any individuals. The important fact is that people with ADHD are complete and valuable members of our communities and workforce.
Dyslexia Awareness Week
by Emma Chalmers, DEN co-chair
October 2024
Dyslexia awareness week is the 2nd to the 8th of October, and I thought I’d focus my blog this week on that.
Firstly- what is dyslexia? Well NHS Inform speak of it this way- ‘Dyslexia is a common learning difficulty that mainly causes problems with reading, writing and spelling. It’s a specific learning difficulty, which means it causes problems with certain abilities used for learning, such as reading and writing. Unlike a learning disability, intelligence isn’t affected. It’s estimated up to 1 in every 10 people in the UK has some degree of dyslexia. Dyslexia is a lifelong problem that can present challenges on a daily basis, but support is available to improve reading and writing skills and help those with the problem be successful at school and work’.
1 in 10. For an average sized hospital ward, that could be 3 to 5 of your colleagues. It’s more prevalent than I believe most people realise.
Now, I want to preface the remainder of this blog by saying that I don’t have dyslexia and am in no way speaking for those who do. My mum and my partner both have it and I want to discuss it from the perspective of someone alongside it, not embedded with it. So, these are my thoughts and experiences.
My mum is an exceptionally intelligent woman who, before she retired, ran a special educational needs department in a mainstream school and had many qualifications under her belt. She also had to do all this without any additional support until she was at university the second time (I was about 8 or so). All through school she was treated as though she was not smart enough because her papers would always come back with red pen marking all over them. The dreaded red pen. Even in my own work in education now I never use red for feedback, based on the negativity felt by my mum. Imagine really knowing your stuff but because the spelling wasn’t correct, you were marked down or failed? And with it being consistent, why did no one consider that there may be an underlying problem?
I remember when she was writing her essays for her second degree. She would hand write it all first then use our very high tech (at the time) Othello computer’s word processor to type it up for printing. She would struggle to read the words on the paper, type them and ensure they were spelled correctly all at the same time. So here comes little helpful Emma who would read out loud the words to be typed as her auditory processing was much better. I improved my reading skills and mum was able to write essays with less frustration. Honestly, nowadays I’m pretty convinced she let me do that so that I was out of trouble, but it was my first understanding that people learn or process information differently to each other.
Did you know that all our posters, printing, presentations, written word, and anything else that is going to be published either in paper form or online needs to be dyslexia friendly? I’m not sure how many people outside of the patient info group know this. You can find out more from the British Dyslexia Association at this link (Dyslexia friendly style guide – British Dyslexia Association (bdadyslexia.org.uk)) but be aware of this if you’re writing anything. Don’t remove screen covers if they are on computers as these can help when trying to read on white backgrounds (all our Word docs!) on screens.
I bet a bunch of you cursed the recycled beige paper that we got a few years ago for printing. I heard many people saying it looks cheap or unprofessional. Now that might be your opinion, but I’ll tell you this one thing- it’s much easier for our dyslexic peers to read!
So, the next time you see something printed in Comic Sans MS and on pink paper, maybe consider that it isn’t childlike or unprofessional but is actually an accessibility need for 1 in 10 of our peers and we should embrace it.
To end, I will give you a wee joke from my mum, because, as she says sometimes ‘if you don’t laugh, you’ll cry’-
My spy movie disappointment
By Emma Chalmers, co-chair of DEN
1 August 2024
CW for movie spoilers
When I was a kid, I was utterly obsessed with Bond movies. Ian Fleming wrote stories that to me showed exotic women, distant tropics and gadgets that woke the geek in me. I religiously watched the films, at least once a fortnight, and knew all the pub quiz answers for the film round at uni.
New spy movies give me so much excitement and I can say that if you name one, I will probably have seen it. That’s not a challenge though so please don’t spam my inbox!
Recently I rewatched Kingsman: The Secret Service. I’d seen it in 2014 when it was released and loved it. This was, however, prior to my overt disabilities and certainly before I became DEN co-chair and pushing for disability advocacy and positive change. So imagine my discomfort when seeing that the two ‘bad guys’ are ‘disabled’. And yet, the actors are not.
Samuel L Jackson plays Richmond Valentine, a megalomaniac who wants to rid the world of excess people to stop climate change. Valentine has a lisp. Jackson does not. I fail to see how adding that ‘character trait’ makes his bad guy any more scary. A lot of the movie is quite tongue in cheek and comic but even with this angle it is once again a lazy way of othering those with disabilities.
Now, had that been Kingsman’s only foray into the lazy disabled villain trope, I might have been able to look past it to an extent. But they made it worse by having Sofia Boutella’s character Gazelle have both lower limbs missing, to be replaced by ‘sword blades’. Yep, the blades that amputee athletes wear to run in. But swords too. Obviously she used these blades to kill people frequently. I actually adore Boutella’s acting (check out Atomic Blond, The Mummy (2017 version, not Brendan’s era) and Star Trek Beyond as some examples of her great acting) but I had to go and google if she was disabled, or at the very least, an amputee. Nope. Not at all. One article I came across lauded the CGI teams on both this movie and Mad Max: Fury Road (Charlize Theron’s Furiosa is missing an arm and has a bionic limb) which definitely is great CGI but is just wrong in principle.
You might be asking yourselves why I’m bothered about this. This is why. Instead of employing disabled actors, or those with amputations or missing limbs, studios would rather spend masses more money on ‘disabling’ the non-disabled. It happens far too often and is not challenged enough. I could speak about so many other characters and I’m sure you could think of some too, like Professor Xavier of the X-Men franchise- neither Patrick Stewart nor James McAvoy are wheelchair users. Another article I read had a great point on this. Studios will often argue that they need the character to walk as their becoming a wheelchair user is a plotline. However, if you can make Chris Evans look like a 90lb man for a few scenes in Captain America, then you can damn well apply the same principle the other way.
Why is it ok for studios to use our disabilities in a way that is convenient to them but not to then use talent that also suits your need for a disabled character? Are our disabilities honestly only seen as plot lines? Can the non-disabled seriously think it’s alright for everyone to bury their heads in the sand on this? When a studio does use a disabled actor for the role of a disabled character, they are celebrated for being so forward thinking and inclusive. But if TV and film were just fully inclusive, that celebration would be unnecessary. As it stands right now, that celebration leaves me with a bad taste in my mouth and an uncomfortable feeling in my gut that really isn’t down to my IBS.
The writing had certainly not covered even 1% of the times that studios choose non-disabled actors over disabled actors and I’m sure you all can think of others. Next time you see the disabled villain trope, or even the disabled good guy played by a non-disabled actor, ask yourself if watching that movie is a form of ignorance around accessibility. Or perhaps, talk about this issue with friends and family to open up more eyes to our plight.
I’ll keep watching my spy movies because I love them. But I’ll happily complain about and condemn the use of my people as easy writing shortcuts. Because I’m anything but quiet.
Ps- if you want to see me and Jack discussing how the disabled villain trope links into ableism and eugenics, then please watch our Let’s Talk About Eugenics lecture from Dec 2023 on the DEN intranet page.
Pps- Sean Connery was of course the best bond and I’ll defend that stance until my dying breath!
How does advocating for others lead to advocating for myself?
9 July 2024
By Emma Chalmers, DEN co-chair
A little bit about me before we start. I am a nurse by trade, but I now teach nurses. I have been disabled all my life but only discovered this in my mid-30s and I have almost exclusively used a wheelchair since 2021. As a nurse, my world was advocating for my patients – ensuring their wishes were heard and acted upon, supporting their loved ones and keeping my team together as best I could. When my occupational health consultant told me that I could no longer work clinically I grieved. I had to feel that loss to then be able to move on. But that is a blog for another day.
My job now as amazing. I still help patients but in a more background manner. Working Monday to Thursday helps me to pace and conserve energy. And I also have more free time for other pursuits- including becoming co-chair of the Disabled Employee Network. This role allows me to advocate for a new group of people- but with skills I have learned in the past.
So, to the point. You may be asking, ‘but Emma, how can you advocate for others if you can’t advocate for yourself?’ Which is a fair question. In my prior life, I sympathised but couldn’t empathise with the patients because although I knew medically what they were experiencing, I never had a cancer diagnosis myself so I couldn’t know what they were going through. This is how I approach DEN advocacy- each person’s disability is individual to them, but even if there was a person with identical disabilities to me, I still wouldn’t know their own personal experience. We are our own experts.
Another thing that I think some readers will recognise is our ability to push for the rights of others, to help others as much as we can but to not apply that same activism to our own selves. An example for you- about a year ago I applied for a post. On the application it asks if you see yourself as being disabled and then what reasonable adjustments you need. I asked for a wheelchair accessible room, focusing on my physical needs, but I forgot entirely that I also struggle with word finding, auditory processing and would also require the questions in advance. The irony? I had advised someone of this exact right not 3 weeks prior!
The retrospective light bulb moments of being disabled can be enormously frustrating but you can be sure that if I ever apply for another job, I’ll be asking for every reasonable adjustment I can get! When I research policy etc to advise our DEN members, I often discover that the same can be applied to myself and in this way, I am learning to advocate more for myself. I often use the expression ‘You cannot pour from an empty cup’ and I need to learn this for myself sometimes. Helping people is ingrained in my whole being, but so is being a disabled person and both are allowed to exist within me.
The TL:DR- advocacy is an incredible gift and one we must give to ourselves as well as others.












